Intro.
The cardiac cycle is the series of events that occur from the end of one heart beat to the beginning of the next. There is a delay of 0.1 seconds in the conduction of the impulse from the atria to the ventricles. This is to allow the atria to contract first, providing adequate time for ventricular filling as the atria act as priming pumps for the ventricles, which provide the main pumping power of the heart.
Blood normally flows from the great vessels through the atria straight into the ventricles, providing 70-75% filling. Atrial contraction provides the remaining 25-30% of blood. (the heart can function without atrial contraction.)
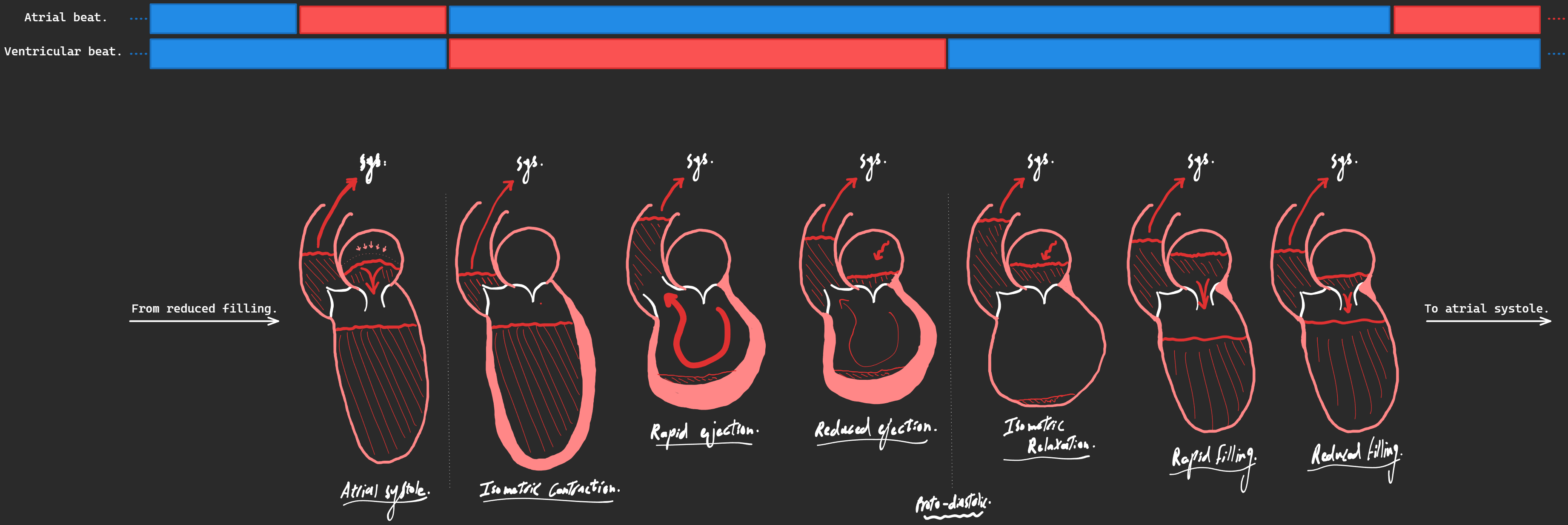
The cardiac cycle lasts 0.8 seconds at a HR of 75 bpm. It goes as follows: atrial systole -⇒ ventricular systole (Iso. contraction, Max. ejection, Reduced ejection.) -⇒ diastole of the whole heart (Proto-diastolic, Iso. relaxation, Rapid filling, Reduced filling.)
(Both sides of the heart have the same mechanical events, but we’re going to focus mostly on the left high pressure side.)
Atrial systole.
- Lasts for 0.1 seconds.
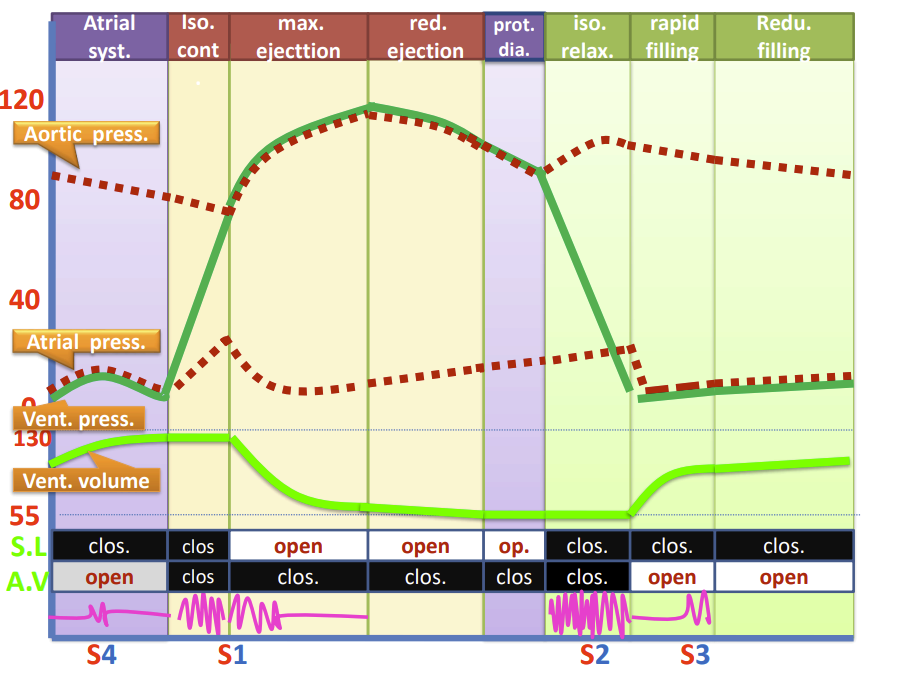
- AV: opened & SL: closed.
- Atrial pressure increases slightly then decreases. (blood escapes from atria to ventricles.)
- Ventricular pressure increases slightly then decreased. (as it accommodates blood from atria.) (its already 70% full before atrial contraction.)
- Aortic pressure decreases. (no blood is being pumped to it, blood is constantly being taken up by peripheral tissue.)
Ventricular systole.
Isometric contraction phase.
- Lasts for 0.05 seconds.
- AV: closed & SL: closed.
- Atrial pressure increases. (AV valve bulges into atrial cavity.)
- Ventricular pressure increases to 80 mmHg.
- Aortic pressure decreases. (no blood is being pumped to it, blood is constantly being taken up by peripheral tissue.)
Rapid ejection phase.
- Lasts for 0.15 seconds.
- AV: closed & SL: opened.
- Atrial pressure decreases. (AV valve pulled down by papillary muscles.)
- Ventricular pressure increases to maximum of 120 mmHg.
- Aortic pressure increases to maximum of 120 mmHg . (blood entry into aorta > blood exit to peripheral tissue.)
Reduced ejection phase.
- Lasts for 0.1 seconds.
- AV: closed & SL: opened.
- Atrial pressure increases. (venous return increases.)
- Ventricular pressure decreases slightly.
- Aortic pressure decreases. (blood entry into aorta < blood exit to peripheral tissue.)
Ventricular diastole.
During late ventricular diastole, atrial diastole also occurs.
Proto-diastolic phase.
- Lasts for 0.04 seconds.
- AV: closed & SL: open (but will close at the end of this phase.)
- Atrial pressure is still increasing.
- Ventricular pressure decreases.
- Aortic pressure decreases.
(This phase is basically the same as the previous phase, the ventricular muscles stop contracting and use the 0.04 seconds as rest time.)
Isometric relaxation phase.
- Lasts 0.06 seconds.
- AV: closed & SL: closed.
- Atrial pressure still increasing.
- Ventricular pressure decreases.
- Aortic pressure increases slightly. (elastic recoil of aorta.)
Rapid filling phase.
- Lasts 0.1 seconds.
- AV: open & SL: closed.
- Atrial pressure decreases. (as blood flows through atrium to ventricles.)
- Ventricular pressure unchanged.
- Aortic pressure decreases.
Reduced filling phase.
- Lasts 0.2 seconds.
- AV: open & SL: closed.
- Atrial pressure still decreasing.
- Ventricular pressure gradual increase.
- Aortic pressure decreases. (blood entry into aorta < blood exit to peripheral tissue.)
(Notice how the chambers that are connected by open valves have the same pressures.) (Proto-diastolic phase is just a continuation of the previous reduced ejection phase.) (The atrial and ventricular pressures rise suddenly because the ventricle contracts without shortening, causing it to build up pressure which pushes on the AV valve bulging it into the atrium, increasing its pressure. The pressure inside the ventricle keeps rising until it surpasses the pressure inside the aorta after which the aortic valve opens.) (In the beginning of the isometric relaxation phase, the aortic pressure rises suddenly due to the elasticity of the aorta causing a back-pressure wave.)