Structures in contractile cardiac muscle cells that aid in contraction.
T-tubules.
- More developed than those of skeletal muscle.
- Located at Z-line.
- Has DHP receptors. (voltage gated Ca++ channels.)
Sarcoplasmic reticulum.
- Simple, less developed.
- Less Ca++ storage than skeletal muscle.
- Has Ryanodine receptors. (ligand gated Ca++ channels.)
Mechanism of contraction.
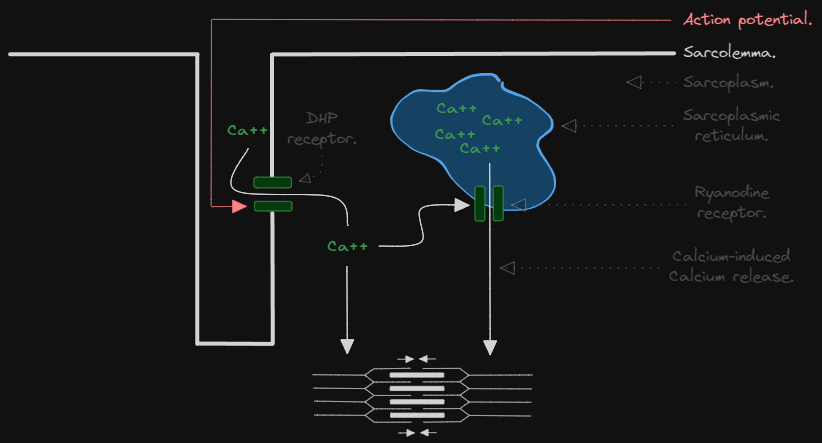
Excitation-Contraction coupling.
- AP (the signal from the pacemaker) spreads along the T-tubules, activating DHP receptors (voltage gated Ca++ channels) causing influx of Ca++ into the cell from ECF. (this is all after phase 0 and phase 1 of electrical activity have been completed.)
- The influx of Ca++ does 2 things:
- It facilitates the release of stored sarcoplasmic Ca++.
- It contributes to the Ca++ required for contraction as described below.
- Force of contraction is proportional to concentration of cytosolic Ca++.
How does Ca++ cause contraction?
- Ca++ binds to troponin C causing a conformational change in the filaments.
- The conformational change reveals a myosin binding site on actin filaments.
- Myosin binds to actin and bends at its hinge region causing shortening of sarcomeres and thus contraction of muscle.
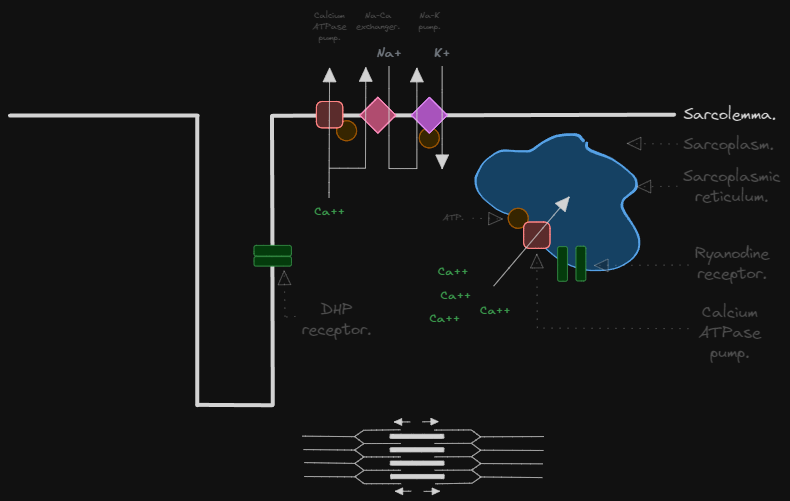
Mechanism of relaxation.
Can be done by 2 processes:
Process 1: Reuptake.
- 80% of Ca++ is actively taken back up into the sarcoplasmic reticulum by action of Ca++ ATPase pump.
Process 2: ECF Ca pumping.
- 20% of Ca++ is pumped out of the cell back into the ECF by action of a Na+-Ca++ exchanger or Ca++ ATPase pump.
- The Na+ that is pumped in is repumped back out using a conventional Na+-K+ pump.
(Note that the pumping of ions follows the electrical activity graph. At first, Na enters the cell to initiate the contraction since it cannot sustain it. K exits the cell to repolarize but is counteracted by influx of Ca. Ca influx stops and K repolarizes the cell. At the end Ca and Na are pumped back out from the cell into the ECF and K is pumped back into the cell.)